Since 2011, I have been a Certified Lymphedema Therapist (CLT) with advanced credentials. For several years, I worked as a medical massage therapist in an integrative health care center treating patients with chronic pain and chronic illness. These people are often challenged by high pain associated with chronic conditions including hypermobility disorders such as the diagnosis of hypermobile Ehlers-Danlos Syndrome (hEDS). Over time, I started to notice that the hEDS women I treated often presented with the characteristic Lipedema fat distribution. And about that same time, there started to be a recognition in the world of vascular and lymphatic therapies that these conditions do indeed have some correlation. I wrote this article a few years ago, and with the current Lipedema Awareness Month, thought to review it. Research is ongoing, support groups and public awareness multiplied, but still so much more is needed.
In 2022, I wrote and presented a case report at an international conference on one patient who originally came to me knowing she and her family members had hEDS. She had been living with a high level of pain, easy bruising, chronic inflammation, fatigue and digestive difficulties, and she sought my services after an emergency colon surgery had resulted in lymphedema of her lower legs.
Using Complete Decongestive Therapy (CDT), the accepted standard of care for the treatment of Lymphedema, her post-surgical leg swelling was reduced and managed. But then we started to notice that she had other features that suggested that her lymphatic disorder was more systemic. With this recognition and involving an integrative team including massage and physical therapies and pain-focused psychology, this patient learned to manage the anxiety related to her diagnoses and daily physical challenges, and to find strategies to reduce pain, exercise effectively and to use compression to support her sense of well-being.
She also obtained a Sequential Pneumatic Compression Device (PCD), like the AIROS 8P and uses it daily. She received care from a CLT massage therapist regularly. Eventually, she even engaged in surgery to remove some of the excess fat tissue. This specialized liposuction was done by a surgeon trained in and utilizing techniques that are specific to address her condition. So far, this has resulted in a much higher quality of life with less pain and increased function. Not only is she happier with the way she looks but she truly has more stamina for the things she loves to do and is now able to reap other benefits from massage and Manual Lymphatic Drainage (MLD) than simply
managing pain and reducing edema.
In my role as a medical massage therapist, I am not promoting surgery as a method that is appropriate for most patients. Many may find the cost prohibitive, and that their insurance does not see this as a wellness option but merely cosmetic. Some patients find that the time to recuperate is simply not available to them. Others find that despite all the challenges associated, the potential for life improvement is worth the costs-time, money, risk and downtime for recuperation. My job is to try to figure out everything I can do with my hands and knowledge as a CLT to help my patients maximize their quality of life. And massage is one of the very wonderful tools that we can offer; it is non-invasive, does not require medication, and has a variety of effects that can be pain reducing in the short and long term. PCDs can mimic the effects of MLD and massage with similar results, although without the benefit of personal connection with a caring professional.
———————————————————————————–
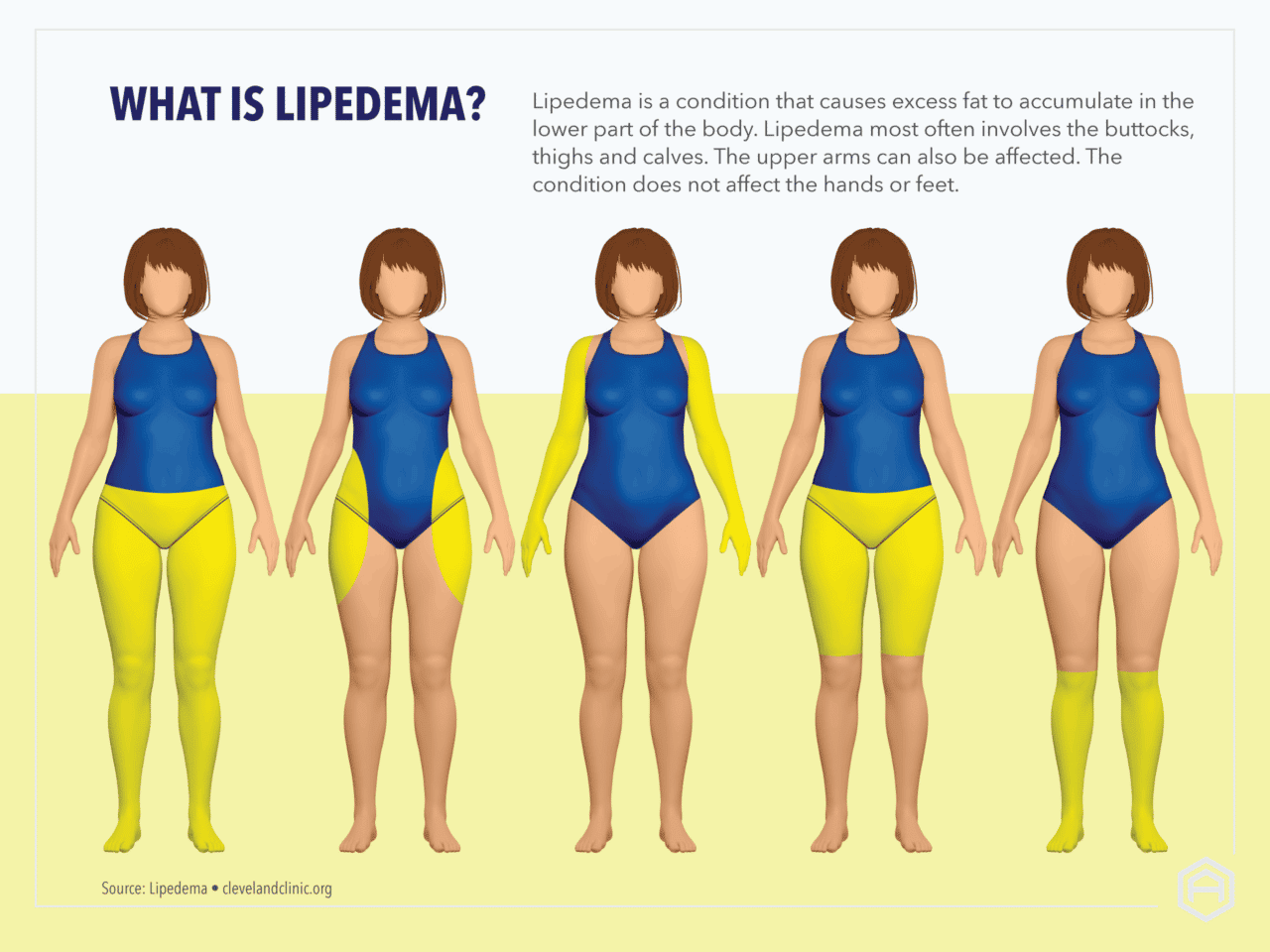
Lipedema, often referred to as the “painful fat disease” is frequently unrecognized, undiagnosed or mistaken for other concerns such as non-lipedemic obesity, fibromyalgia, or Lymphedema. This loose connective tissue disorder1 is seen almost exclusively in females, and some specialists, such as Dr Paula Stewart, have postulated that it is a genetic expression of the desirable survival traits for early humans, a “mother of the species” image such as is often seen in ancient fertility symbols. The fat distribution, in general noted to be symmetrical and bilateral and usually concentrated in the legs, hips and buttocks, is a characteristic look noted in these ancient depictions and sacred objects. Interestingly, metabolic disease is not usually associated with this condition. Although it does frequently, but not always, progress to obesity, these patients generally do not have associated high blood pressure, high lipids or type II diabetes, but they often do have other connective disorders such as hypermobility.
Interestingly, metabolic disease is not usually associated with this condition. Although it does frequently, but not always, progress to obesity, these patients generally do not have associated high blood pressure, high lipids or type II diabetes, but they often do have other connective disorders such as hypermobility. Women with Lipedema may have a constellation of concerns including easy bruising, hypersensitivity to touch, nodules in the fat tissue that are sore and cause a rippled appearance and weight gain that is not responsive to traditional dieting. Uncontrolled and undiagnosed Lipedema may lead to Lymphedema. Other challenges that may be associated with connective tissue abnormalities including joint pain, overactive immune response known as Mast Cell Activation Syndrome (MCAS) and autonomic dysregulation known as Postural Orthostatic Tachycardia Syndrome (POTS) can also
be present. These various concerns make treatment and self-management extra tricky. Interestingly, Lipedema is often exacerbated at times of hormone change such as puberty, pregnancy or menopause, and ongoing research is looking into the importance of estrogen in the exacerbation of the condition.
Lipedema also seems to be inherited. Recently, a gene has been identified that has to do with progesterone regulation and is implicated as a potential instrument in thedevelopment of Lipedema. Mother/daughter patient populations are being studied. More research results around the genetic and hormonal influences are surely imminent.
What is it about Lipedema that leads to so much pain? While not fully clear, there are factors that are suggestive.
Imaging studies and tissue samples are showing that there is indeed a difference in the lymphatic and tissue structures beyond the external appearance; this is key to learning more about the causes of pain and dysfunction. Some things we do know include that edema in any setting is often painful. Lymphatic fluid is associated with inflammation, which is great for healing an acute illness or injury but is irritating to our systems and the
delicate nerve structures upon which it puts pressure when it is unresolved. The extra fluid, even if not associated with increased fat buildup, is heavy and wearing on the joint structure. The fluid is extra work for the vascular and lymphatic systems and that can be generally fatiguing. When we are fatigued, we tend to be more susceptible to pain. In an article published in 2021, pain in lipedema is reported to be likely due to overactive signaling of the sympathetic nervous system and triggered by hormonal and genetic factors.
These challenges to a general sense of wellbeing may also have a mental health impact. There is a high incidence of depression and anxiety among these patients which may be a result of the pain, fatigue, and body image as well as a sense that there is no clear management strategy if they are even lucky enough to get a difficult-to-obtain diagnosis. Fat-shaming is a big problem and adds to the emotional impact. For example, at an international conference that I attended a few years ago, I was personally shocked as I witnessed a renowned doctor basically shout at a lipedema patient that she should “simply accept the fact that you are fat”! While later that day, another presentation showed images of normal obesity fat samples next to those of lipedema patients, and there was a very clear difference. Awareness and acceptance will take a long time to be fully appreciated and integrated in the national and international medical communities.
There are no known medications specific to treatment of lipedema, so medical management is focused on reducing pain, inflammation, fibrosis and edema. Patients with lipedema should consider and discuss with their providers whether any of the medications that they may be taking for other conditions tend to increase edema as this can worsen symptoms. Diuretics are potentially exacerbating as they do not address inflammation and may make it more difficult for the lymphatic system to process the proinflammatory proteins that can create a viscous cycle and possibly lead to the development of a secondary lymphedema, known as Lipo-lymphedema, in these
patients. Research is ongoing to seek oral or injectable medications and there appears to be some promise in the use of GLP1s, which are proving so revolutionary in so many settings, but more study is required and these are not appropriate for everyone. As with all medications, there is the possibility of unfortunate side effects.
So, in the meantime, we must manage Lipedema with compassion and without judgement and simply address the fact that all persons deserve to have the best possible quality of life. My job as I see it is to be an advocate in addition to my hands-on interventions and to offer ideas and strategies to patients that will help them reduce pain and increase function. I seek to offer ideas and resources to connections that may assist with diet, exercise and mental health support as well as daily self-management strategies such as compression garments, skin care and tools for home use including Sequential Pneumatic Compression Devices (PCD) like our AIROS pumps.
————————————————————————————–
Massage therapy is an out-of-pocket expense and not in the regular budget for most patients, while PCD therapy can be available on demand, daily, at home. As an adjunct to daily-wear compression garments that massage and support the tissues while the patient is awake, and in addition to the education that a qualified lymphatic therapy specialist can offer, at AIROS we try to support the very best quality of life that those living with lipedema, as with any other chronic condition, can achieve. Please reach out o me with any questions, comments or concerns; I am always eager to talk with you!
Adie MacKenzie, PTA, LMT, CLT-LANA, NBC-HWC
amackenzie@airosmedical.com
———————————————————————————–
- Herbst KL, Kahn LA, Iker E, Ehrlich C, Wright T, McHutchison L, Schwartz J, Sleigh M, Donahue PM, Lisson KH, Faris T, Miller J, Lontok E, Schwartz MS, Dean SM, Bartholomew JR, Armour P, Correa-Perez M, Pennings N, Wallace
EL, Larson E. Standard of care for lipedema in the United States. Phlebology. 2021 Dec;36 (10):779-796. doi: 10.1177/02683555211015887. Epub 2021 May 28. PMID: 34049453; PMCID: PMC8652358. - Aksoy H, Karadag AS, Wollina U. Cause and management of lipedema-associated pain. Dermatol Ther. 2021 Jan;34(1):e14364. doi: 10.1111/dth.14364. Epub 2020 Oct 12. PMID: 33001552.
- Mohseni, Yasmine BS*,†; Vazirnia, Aria MD†; Minokadeh, Ardalan MD, PhD‡; Amron, David M. MD†; Coleman, William P. III MD§. Targeting Inflammation and Fibrosis in Lipedema: The Potential Role of Glucagon-like Peptide-Receptor Agonist Therapies. Dermatologic Surgery 52(6S):p S72-S75, June 2026. | DOI: 10.1097/DSS.0000000000005172